Neck Stiffness with Arm Numbness or Tingling. Could It Be Cervical Disc?
Numbness and pain running from neck to arm. Find out the real cause.
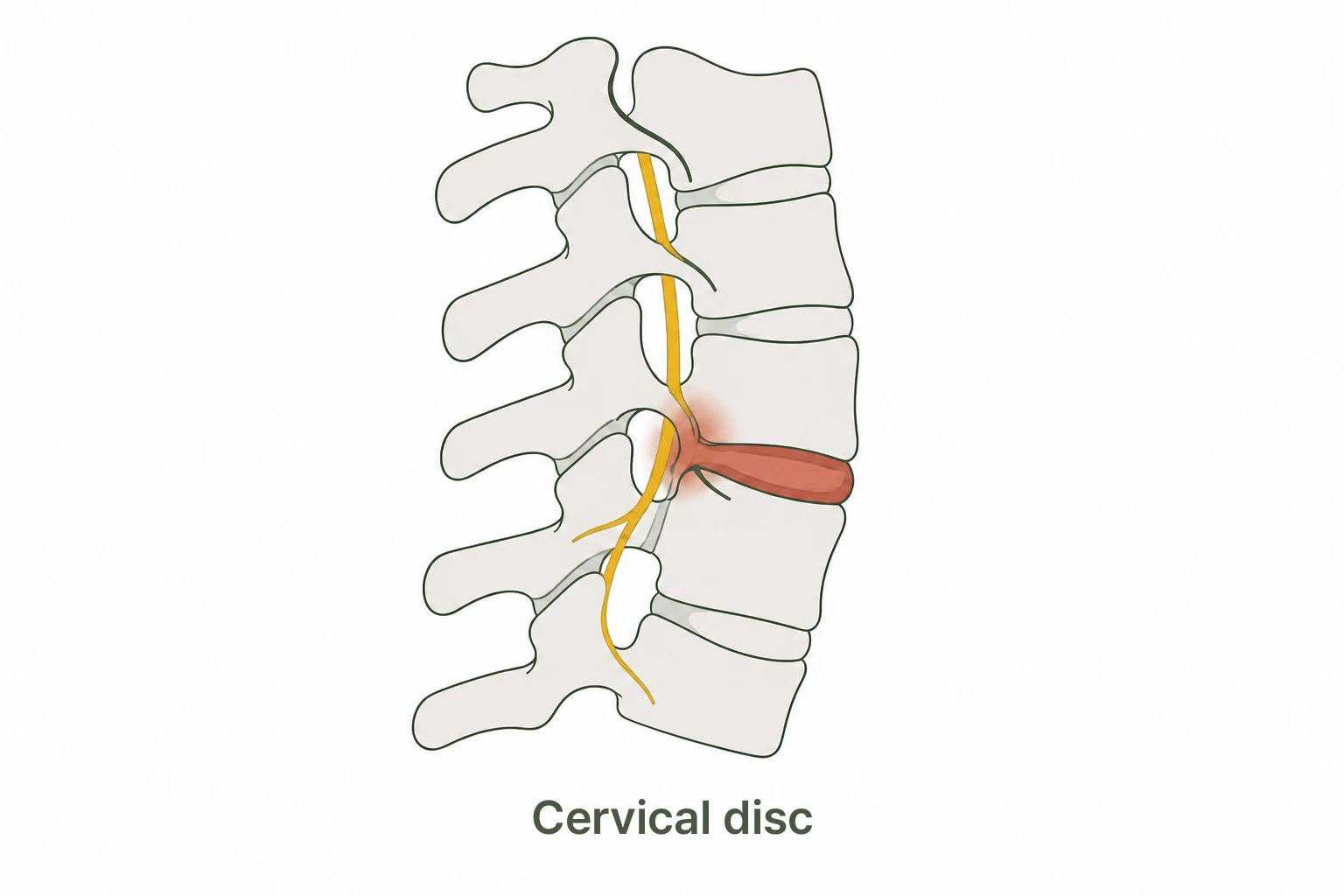
Your neck feels stiff and one arm or certain fingers tingle or go numb. Symptoms may shift when you move your head. Cervical disc herniation occurs when the disc material between neck vertebrae presses on nearby nerves. Accurate assessment comes first.
Quick Answer: Cervical disc herniation occurs when the disc nucleus protrudes between neck vertebrae and irritates a nerve. We begin with a gait analysis to assess movement changes, then use a three-stage Circulation Therapy that calms the irritated nerve, rebuilds weakened muscles, and integrates healthy movement. A disc visible on MRI may not be causing pain, and pain can exist even when imaging looks normal.
Seek medical attention immediately if:
- Sudden weakness or paralysis in an arm
- Numbness in both arms and legs at the same time
- Unsteady gait or loss of balance
- Bladder or bowel dysfunction
These symptoms may suggest cervical disc herniation
- Neck and shoulder pain, with a heavy, stiff neck. A dull ache in the back of the neck extends to the shoulder.
- Numbness or tingling in one arm or fingers. It radiates into the whole arm or specific fingers, depending on which nerve is involved.
- Symptoms worsen with certain head positions. Tilting or extending the neck increases numbness or pain.
- Arm weakness or dropping objects. Nerve compression can reduce grip strength or muscle control.
- Possible headaches. Aching in the back of the head or behind the eyes may accompany neck pain.
Why does cervical disc herniation happen?
Structural cause. The disc nucleus pushes outward (herniates) and presses on a nerve root, causing pain and numbness. Prolonged forward head posture concentrates load on the lower cervical joints, accelerating disc damage.
Nerve sensitivity. When a nerve is irritated, pain signals are amplified. The same disc change can cause very different symptoms depending on how sensitive the nervous system is.
Imaging and symptoms don’t always match. Disc changes on MRI may cause no pain at all, while imaging can look normal with significant pain. Functional movement assessment alongside imaging gives the full picture.
Forward Head Posture and Cervical Disc
- Each 2.5 cm of forward head adds ~4.5 kg of load on the neck
- Prolonged phone and computer use is a key risk factor
- Lower cervical discs (C5-C7) bear the most load
- Posture correction is central to prevention and avoiding recurrence
Simple self-check
If your symptoms change in these situations, cervical nerve involvement is possible. Accurate diagnosis requires professional evaluation.
- Tilting your head toward the painful side. Does arm numbness worsen or pain increase?
- Gently lifting your head with your hands. If arm numbness decreases, this may suggest cervical nerve compression.
- Raising your arm above your head. If numbness actually reduces, this can also indicate a cervical nerve pattern.
Is it a cervical disc, or another neck or shoulder problem?
Arm numbness starting in the neck is not always a cervical disc herniation. Forward head posture (myofascial pain) and thoracic outlet syndrome can produce overlapping symptoms.
Cervical Disc Herniation
- Numbness or tingling runs from one side of the neck down the arm to the fingers
- Symptoms shift when you move your head to different positions
- Possible arm weakness or sensory loss
- Spurling’s test (axial compression) may be positive
Forward Head Posture / Myofascial Pain
- General aching in both sides of the neck and shoulders
- Any arm tingling does not extend clearly to the fingertips
- Temporarily relieved by posture correction or stretching
- Muscles feel knotted and tender on palpation
Thoracic outlet syndrome (TOS) is another cause of arm numbness. If raising the arm overhead intensifies tingling, or there is tenderness below the clavicle, TOS should also be evaluated. Even when MRI shows a disc abnormality, it may not be the actual source of your symptoms. Clinical assessment remains essential.
Our Approach at Yonsei SM Pain Clinic
Surgery is rarely necessary for cervical disc herniation. The key is improving the environment around the nerve and restoring weakened muscles to relieve symptoms.
- Phase 1: Calm (Circulation HD)
Reduce tension in neck muscles and inflammation around the nerve. Trigger point injections and fascial hydrodissection release tense muscles and fascial adhesions. - Phase 2: Activate (Circulation PT)
Restore weakened deep cervical flexors and shoulder stabilizers. Movement correction trains posture patterns that reduce load on the neck. - Phase 3: Integrate
Train natural, healthy neck posture in everyday movement. Lifestyle habit correction is included to reduce recurrence risk.
Why don’t we look only at the neck?
Excessive pressure on the cervical disc often originates not just in the neck itself, but in the thoracic spine and pelvis. When the thoracic spine is stiff, the neck has to compensate by moving more, increasing disc stress. When pelvic alignment is off, the curves of the entire spine (lumbar, thoracic, and cervical) shift, raising the load on the cervical discs. That is why at Yonsei SM Pain Clinic, we evaluate thoracic and pelvic alignment together as part of every cervical disc assessment.
Frequently Asked Questions
My MRI shows a disc herniation. Do I need surgery?
MRI confirmation of disc herniation does not mean surgery is required. Unless there is severe arm paralysis or bladder or bowel dysfunction, conservative treatment is tried first. With the right environment, disc material can often resorb naturally over time. Normal MRI but in pain Q&A →
How do I know if it’s my neck disc or a shoulder problem?
Cervical disc issues often cause numbness or tingling in a specific arm pattern, and symptoms shift with head position. Shoulder problems tend to focus pain at the shoulder joint itself, especially when lifting the arm. Both can occur together, so thorough evaluation is important.
What positions are bad for cervical disc?
Forward head posture, prolonged downward neck flexion (phone use), and keeping the neck twisted in one position all increase load on the lower cervical discs. Adjusting monitor and chair heights helps significantly. Posture Correction Q&A →
What kind of pillow should I use?
Height matters more than material. The pillow should maintain the natural C-curve of the neck, not too high and not too low. Side sleepers and back sleepers need different heights to avoid accumulating neck tension during sleep. Pillow Selection Q&A →
How long will treatment take?
Duration depends on how long symptoms have been present, their severity, and daily postural habits. Acute cases (within 2-4 weeks of onset) often improve quickly. Longer-standing symptoms take more time. Changing habits alongside treatment has a significant impact on outcomes. Treatment Duration Q&A →
I’m nervous about injections. Are they necessary?
Circulation HD is different from nerve block injections. It uses fine needles to release tense muscles and fascial adhesions, aiding pain relief and functional recovery. Treatment direction is decided together based on your condition and preferences. Injection Treatment Q&A →
References
- Childress MA, Becker BA. Nonoperative management of cervical radiculopathy. Am Fam Physician. 2016;93(9):746-754.
- Thoomes EJ et al. The effectiveness of conservative treatment for patients with cervical radiculopathy: a systematic review. Clin J Pain. 2013;29(12):1073-1086.
- Caridi JM, Pumberger M, Hughes AP. Cervical radiculopathy: a review. HSS J. 2011;7(3):265-272. PMC3192889
- Nikolaidis I, Fouyas IP, Sandercock PA, Statham PF. Surgery for cervical radiculopathy or myelopathy. Cochrane Database Syst Rev. 2010;(1):CD001466. PMID 20091520
- Quek J, Pua YH, Clark RA, Bryant AL. Effects of thoracic kyphosis and forward head posture on cervical range of motion in older adults. Man Ther. 2013;18(1):65-71. PMID 22959228
- Legaye J, Duval-Beaupere G, Hecquet J, Marty C. Pelvic incidence: a fundamental pelvic parameter for three-dimensional regulation of spinal sagittal curves. Eur Spine J. 1998;7(2):99-103. PMID 9629932
- Roussouly P, Pinheiro-Franco JL. Biomechanical analysis of the spino-pelvic organization and adaptation in pathology. Eur Spine J. 2011;20(Suppl 5):609-618. PMID 21809016
Related Articles
Stiff neck with arm numbness or tingling?
We begin with gait analysis to assess movement, then apply a 3-stage Circulation Therapy approach.
3F Cheongdam Building, 413 Hakdong-ro, Gangnam-gu, Seoul (3 min walk from Gangnam-gu Office Station Exit 4)