When pressing deep into your buttock hurts and the pain tingles down your leg
Piriformis syndrome — a buttock muscle is compressing your sciatic nerve.
Your back isn’t really the problem, but pressing deep into the buttock hurts and the leg tingles all the way down. Sitting for a long time pulls at the buttock and the back of the thigh, and crossing your legs makes the tingling worse. Even if your MRI shows no disc herniation, symptoms like these point to piriformis syndrome.
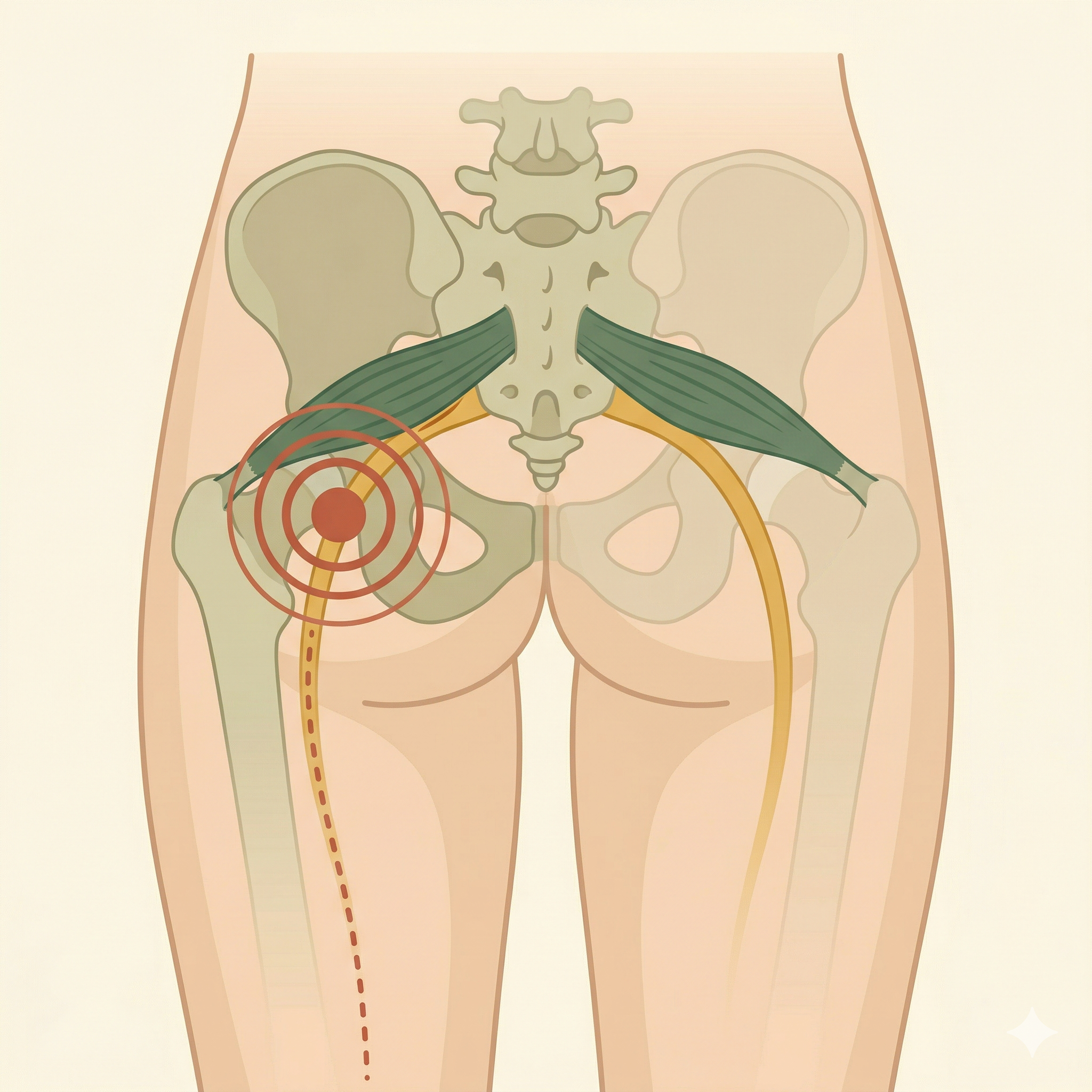
Quick Answer: The piriformis is a small muscle deep in the buttock, lying right on top of the sciatic nerve. When it becomes overly tense or enlarged, it compresses the sciatic nerve, causing buttock pain, leg tingling, and a pulling sensation. It is one of the most common reasons sciatica-type symptoms appear without any disc herniation.
You need a differential evaluation if:
- Night pain persists along with fever → rule out infection or tumor
- Foot drop (the foot droops or you can’t lift your toes) → rule out nerve damage
- Paralysis or numbness in both legs at once → rule out a spinal cord lesion
- Bladder or bowel problems appear together → seek emergency evaluation immediately
3 Key Points on This Page
- What the piriformis is and why it causes sciatica
- How to tell lumbar disc herniation apart from piriformis syndrome
- The Circulation Therapy approach to releasing piriformis tension and restoring pelvic balance
Symptoms that suggest piriformis syndrome
- Pressing deep into the buttock hurts and the pain tingles down the leg — Pressing the center of the buttock with your fingers produces deep tenderness, and the symptoms spread into the leg.
- Sitting for a long time pulls and tingles in the buttock and back of the thigh — In a prolonged sitting position, the piriformis compresses the sciatic nerve and leg symptoms appear.
- Buttock pain when climbing stairs or walking uphill — Movements requiring hip external rotation tighten the piriformis further, increasing the pain.
- The back feels fine, but buttock and leg pain is severe — Symptoms worsen with hip rotation movements rather than with bending the back forward.
- Crossing your legs while seated makes the tingling worse — A crossed-leg position stretches and compresses the piriformis even more, intensifying sciatic nerve compression.
What causes piriformis syndrome
The piriformis is a small muscle running from the sacrum to the greater trochanter of the femur (the bony bump on the outer thigh). Normally it rotates the hip outward. When it becomes overly tense or enlarged, it presses on the sciatic nerve that passes just beneath it, causing pain and tingling.
- Piriformis overactivity — Prolonged sitting, pelvic asymmetry, and crossing the legs keep the piriformis continuously contracted and tense.
- Buttock muscle imbalance — When the glutes (gluteus maximus, medius, and minimus) are weak, the piriformis overcompensates and enlarges.
- Pelvic asymmetry — A height difference between the left and right pelvis creates uneven tension in the piriformis on each side.
Why does it hurt when the MRI is normal?
Even with no disc herniation on MRI, the piriformis can compress the nerve and produce sciatica symptoms. The piriformis itself is not well seen on a standard MRI. Piriformis syndrome is diagnosed through palpation and functional assessment.
- Piriformis syndrome — Deep tenderness in the buttock, worse when crossing the legs, normal with forward back bending
- Lumbar disc herniation — Accompanied by back pain, worse when bending forward, worse when coughing
The two can occur together, so accurate palpation assessment is important.
Our Approach at Yonsei SM
Piriformis syndrome hinges on releasing piriformis tension and correcting buttock muscle imbalance.
- Phase 1: Calm Down
Circulation HD relieves tension and inflammation in the piriformis fascia. By settling the tension around the sciatic nerve, it reduces nerve compression and decreases pain. - Phase 2: Activate (Circulation PT)
We assess the imbalance between the piriformis and the buttock muscles. We intensively activate the weakened glutes (gluteus maximus and medius) and release the overactivity with piriformis stretching. - Phase 3: Integrate
Gait analysis checks the hip rotation pattern while you walk. We correct pelvic stability in sitting and walking so that the load is not concentrated on the piriformis.
Frequently Asked Questions
How do I tell whether it’s piriformis syndrome or a lumbar disc?
If bending the back forward sends pain down the leg, a lumbar disc is the first suspect. On the other hand, if bending the back is fine but pressing deep into the buttock hurts and crossing the legs worsens the tingling, piriformis syndrome is more likely. The two can occur together, so accurate palpation assessment is needed. Sciatica Q&A →
Can I do piriformis stretches on my own?
Piriformis stretches such as the pigeon pose can be helpful, but repeating only stretches without first identifying the cause (weak glutes, pelvic asymmetry) brings only temporary relief. Strengthening the weakened glutes must go hand in hand to reduce recurrence.
Can a buttock injection cure it?
Injections around the piriformis provide temporary pain relief. However, if the underlying cause of the piriformis tension (muscle imbalance, postural habits) isn’t corrected, it often recurs. Circulation Therapy focuses on correcting the root cause along with reducing pain.
I have a job that requires long hours of sitting. Can it fully heal?
People who sit for long periods are prone to recurring piriformis tension. If you correct the cause of the tension and also improve your sitting posture and a habit of stretching regularly, you can reduce recurrence. Even if a complete recovery is difficult, improving daily function is certainly achievable.
Can piriformis syndrome occur together with sacroiliac joint dysfunction?
Yes. When there is pelvic asymmetry, piriformis syndrome and sacroiliac joint dysfunction sometimes appear together. When both problems coexist, it is important to assess the balance of the whole pelvis and build a treatment plan in the right order. Sacroiliac Joint Dysfunction →
Related Articles
First, check whether your buttock pain is compressing the sciatic nerve.
Through palpation assessment and gait analysis, we identify the cause of your piriformis tension and build a personalized treatment plan.
Book OnlineReferences
- Boyajian-O’Neill LA, et al. Diagnosis and management of piriformis syndrome: an osteopathic approach. J Am Osteopath Assoc. 2008;108(11):657–664.
- Hopayian K, et al. The clinical features of the piriformis syndrome: a systematic review. Eur Spine J. 2010;19(12):2095–2109. PMID 20596735
- Tonley JC, et al. Treatment of an individual with piriformis syndrome focusing on hip muscle strengthening and movement reeducation. Phys Ther. 2010;90(8):1240–1252.
- Cassidy L, et al. Piriformis syndrome: implications of anatomical variations, diagnostic techniques, and treatment options. Surg Radiol Anat. 2012;34(6):479–492.