Sudden, Intense Shoulder Pain That Hurts to Touch? It Could Be Calcific Tendinitis
Calcium deposits in the rotator cuff tendons trigger severe acute inflammation.
If your shoulder suddenly became excruciatingly painful, hurts even at the slightest touch, and keeps you awake at night, calcific tendinitis may be the cause. The approach is to first calm the acute pain, then restore shoulder function and reduce recurrence risk.
Quick Answer: Calcific tendinitis occurs when calcium deposits form in the shoulder tendon (most commonly the supraspinatus), triggering acute inflammation and severe pain. Treatment follows three phases, first calming the acute pain, then waking the weakened shoulder muscles and rotator cuff, and finally connecting movements into daily patterns to reduce recurrence risk.
Seek medical attention quickly if:
- Fever, redness, or significant warmth with the pain calls for ruling out septic arthritis, so see a doctor promptly.
- Being unable to lift the arm at all after an injury calls for ruling out a rotator cuff tear.
- Pain lasts more than 2 weeks and keeps worsening
- Numbness or decreased sensation in the arm or hand progressing
3 Key Points on This Page
- Why calcium deposits cause such sudden, severe pain
- How symptoms differ by phase of calcific tendinitis
- Phase-by-phase treatment approach from acute pain to recurrence prevention
These symptoms may suggest calcific tendinitis
- Sudden and intense shoulder pain. The pain intensifies rapidly within a day or two, often worse at night.
- Extreme tenderness to touch. Pressing a specific spot on the shoulder produces severe pain.
- Difficulty moving the arm in any direction. The pain is so severe it restricts movement in all directions.
- Especially painful when lifting or raising the arm sideways. Even simple everyday movements become very difficult.
- Pain that persists for days to weeks. Acute phase pain can last anywhere from a few days to several weeks.
Why does this cause such extreme pain suddenly?
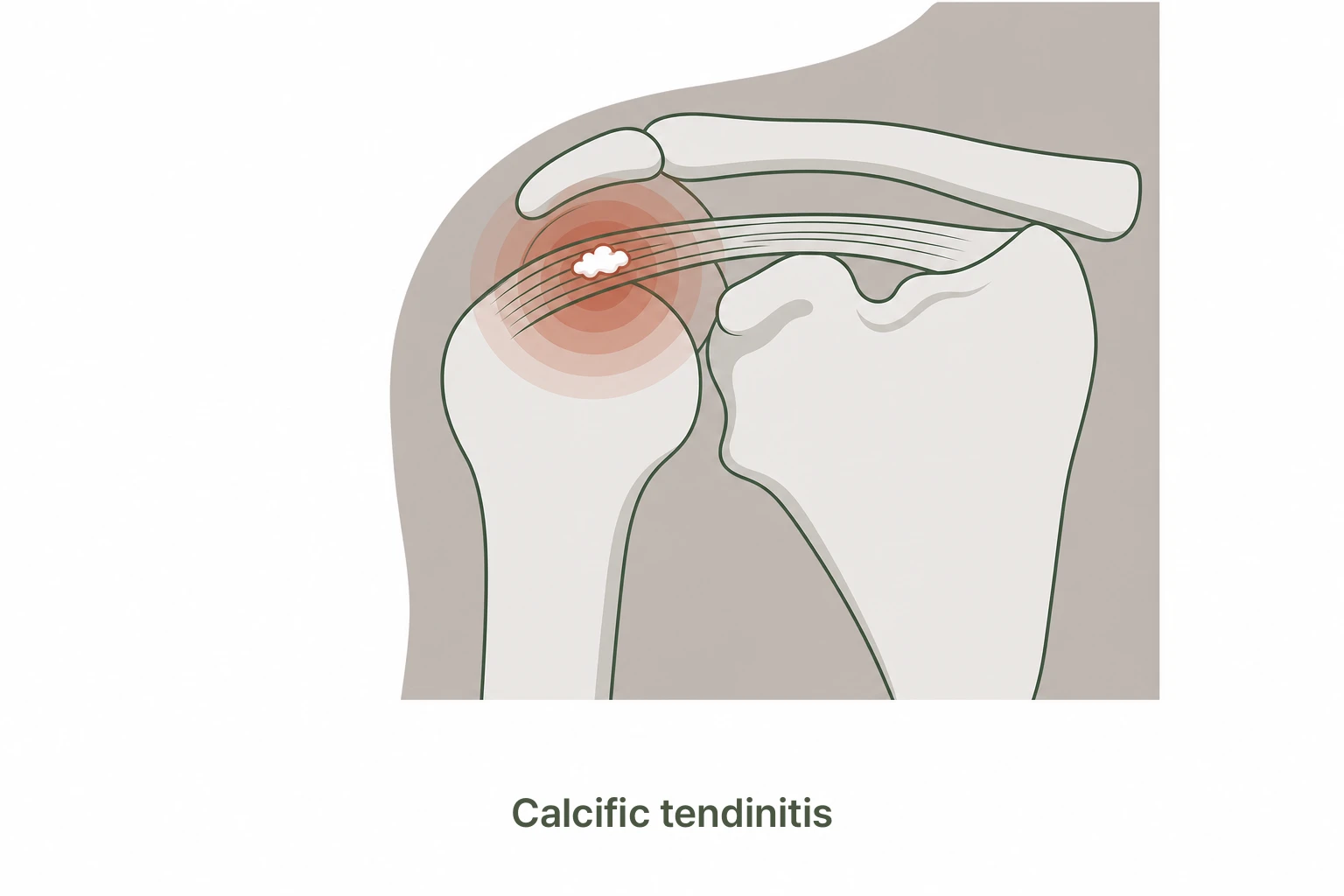
Calcium slowly deposits in the shoulder tendon (most commonly the supraspinatus). This accumulation process itself may cause little or no pain. But at some point, the body recognizes the calcium as a foreign substance and begins trying to remove it, triggering a sudden, intense inflammatory response. This is the source of the excruciating pain.
The rotator cuff tendons have relatively poor blood supply. Once damaged or affected by calcium deposits, recovery can be slow. Repetitive microtrauma and reduced blood flow from overuse are contributing factors that let calcium accumulate over time.
Phases of Calcific Tendinitis
- Formative phase. Calcium begins accumulating in the tendon, with little or no pain.
- Resting phase. The calcium has hardened and may cause mild chronic discomfort.
- Resorptive phase, the acute phase. The body’s inflammatory response to absorb the calcium causes extreme pain. This is the most painful stage.
- Recovery phase. The calcium is absorbed and pain gradually decreases.
Why is the resorptive phase the most painful?
Paradoxically, the process of calcium being absorbed causes the most severe pain. Immune cells flood the area to clear the calcium deposits, triggering an intense inflammatory reaction. The following changes occur during this phase.
- Pain comes on very suddenly and intensely
- Shoulder area may become swollen and warm to the touch
- Night pain is especially severe and can disrupt sleep
The severe acute pain can actually be a signal that calcium is being absorbed, which is a step toward recovery. However, if fever or significant redness accompanies the pain, septic arthritis must be ruled out promptly.
Is it calcific tendinitis, or another shoulder problem?
Sudden, severe shoulder pain with difficulty lifting the arm is not always calcific tendinitis. Rotator cuff tears and frozen shoulder can look similar and need to be distinguished.
Calcific Tendinitis
- Abrupt onset of severe shoulder pain (acute phase)
- Difficulty raising the arm through a specific arc (60-120°)
- Calcium deposit visible on X-ray
- Even minimal movement causes intense pain in the acute phase
Rotator Cuff Tear
- Difficulty raising the arm with noticeable weakness
- Night pain is common. Lying on the shoulder worsens it
- Develops gradually in most cases
- Tendon tear confirmed on ultrasound or MRI
Acute calcific tendinitis can be so severe that it is mistaken for a frozen shoulder or even a septic joint infection. If extreme shoulder pain appears suddenly alongside fever or chills, prompt evaluation is needed to rule out infection.
Our Approach at Yonsei SM Pain Clinic
Treating calcific tendinitis requires a phase-by-phase approach. We first calm the acute pain, then restore shoulder function, and finally address recurrence prevention.
- Phase 1: Calm Down (Circulation HD)
Managing the acute, excruciating pain is the top priority. Circulation HD calms the intense inflammatory response around the tendon. When needed, a precise ultrasound-guided procedure effectively reduces swelling and inflammation. - Phase 2: Wake Up (Circulation PT)
Once calcium has begun absorbing and pain subsides, we work to reactivate the shoulder muscles and rotator cuff weakened by pain and disuse. Movement correction progressively restores shoulder function. - Phase 3: Connect
We train natural, pain-free movement patterns for daily activities. Posture correction and guidance on maintaining shoulder muscle balance help reduce recurrence risk.
Frequently Asked Questions
Can calcific tendinitis heal on its own?
As calcium is naturally absorbed, pain can decrease over time. However, without proper management during the acute phase, recovery can take much longer and shoulder function deficits may persist. Appropriate treatment accelerates recovery. Treatment Duration Q&A →
How is it different from frozen shoulder?
Frozen shoulder involves progressive stiffening of the joint capsule with gradually increasing movement restriction. Calcific tendinitis is characterized by sudden, acute severe pain. Both conditions can coexist, so thorough evaluation is important. Frozen Shoulder Page →
How does it differ from rotator cuff tear?
A rotator cuff tear involves a physical tear in the tendon, while calcific tendinitis involves calcium deposits forming in the tendon. Both affect the shoulder tendons but the cause and treatment approach differ significantly. Rotator Cuff Conditions Page →
Can I exercise my shoulder?
During the acute phase, vigorous exercise should be avoided. Gentle movements within a pain-free range are acceptable. Once pain settles, appropriate movement correction and strengthening exercises can begin. It is safer to establish a tailored routine after assessment. Shoulder Exercise Q&A →
Why is the pain worse at night?
When lying down, pressure distribution around the shoulder changes, and maintaining the same position during sleep can intensify pain perception. Night pain is particularly prominent during the acute phase of calcific tendinitis. Night Pain Q&A →
Is surgery necessary?
The vast majority of cases are managed with non-surgical treatment. Surgery may be considered when there is no response to conservative treatment or when calcium deposits are large and persist for an extended period. Surgery Decision Q&A →
Related Articles
References
- Merolla G et al. Calcific tendinitis of the shoulder. EFORT Open Rev. 2016;1(8):310-316.
- Serafini G et al. Rotator cuff calcific tendinitis: short-term and 10-year outcomes after US-guided percutaneous treatment. Radiology. 2009;252(1):157-164.
- Louwerens JK et al. Comparing ultrasound-guided needling combined with a subacromial corticosteroid injection versus high-energy extracorporeal shockwave therapy for calcific tendinitis of the shoulder. Am J Sports Med. 2016;44(3):635-642.
- Cho NS et al. Radiologic course of symptomatic calcific tendinitis in the shoulder. J Shoulder Elbow Surg. 2010;19(2):185-191.
Shoulder pain so severe you can’t bear to touch it?
We stabilize the acute pain first, then guide you through phase-by-phase shoulder recovery.
Book Online