Back pain with numbness running down your leg?
Lumbar disc herniation — a bulging disc is pressing on a nerve.
It hurts more when you bend forward, and sitting is harder than standing. If your leg also feels numb and tight, a disc may be pressing on a nerve.
Quick answer: In disc herniation, a disc bulges out and irritates a nerve, so back pain and leg numbness can appear together. Rather than drawing conclusions from “imaging findings” alone, it is important to assess the degree of nerve symptoms together with function to decide on the right treatment.
Seek emergency evaluation if you have any of these
- Bowel or bladder dysfunction (possible cauda equina syndrome)
- Sudden weakness in the ankle/toes, or rapid worsening
- Reduced sensation in the perineal area (saddle anesthesia)
- Fever or chills, or rapid worsening after an injury
3 Key Things This Page Covers
- What a lumbar disc herniation is and why it happens
- Why surgery isn’t always needed even when a disc shows up on MRI
- How to manage a disc herniation without surgery
These symptoms may point to a lumbar disc herniation
- Back pain + leg numbness — starts in the back and runs down through the buttock, thigh, and calf.
- Worse when bending — bending forward or sitting for a long time makes it worse.
- A sharp jolt when coughing or sneezing — pain briefly spikes when abdominal pressure rises.
- Discomfort in just one leg — symptoms usually concentrate in one leg.
- Stiff in the morning, better with movement — stiff on waking, then loosens up little by little.
What is a lumbar disc herniation?
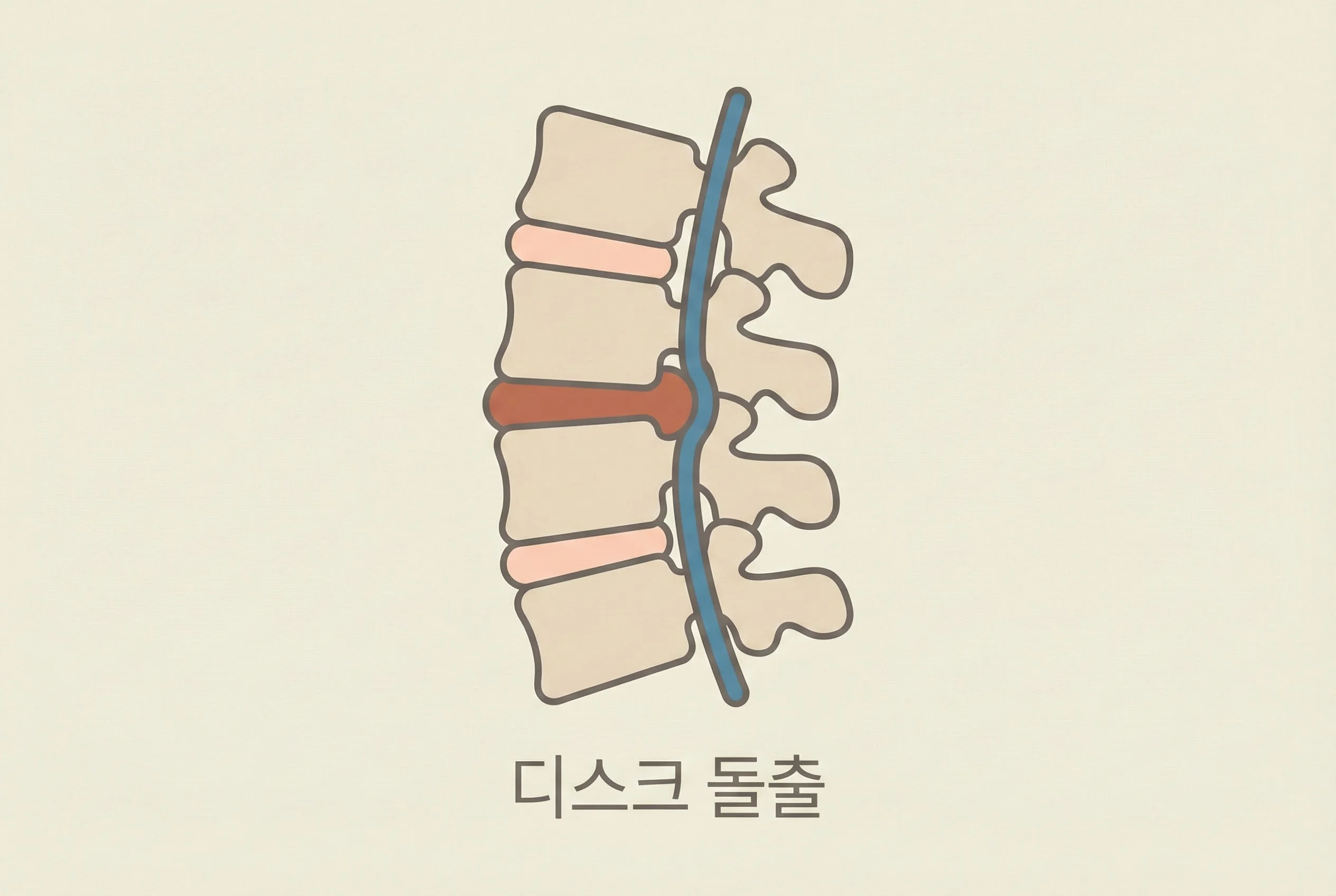
The intervertebral disc is a cushion that absorbs shock between the vertebrae. It consists of a jelly-like inner nucleus pulposus and the annulus fibrosus that surrounds it.
When repeated pressure or poor posture cracks the annulus, the nucleus pushes outward, and when it presses on a nerve, leg numbness and pain occur.
However, a herniated disc can be symptom-free if it isn’t pressing on a nerve, and conversely, even a mild disc problem can cause severe pain because of inflammation.
Stages of disc herniation
- Bulging — the disc swells outward
- Protrusion — part of the disc pushes out
- Extrusion — the nucleus breaks through the annulus
- Sequestration — the herniated fragment separates
Herniated disc = surgery? Not necessarily
Many studies report that a herniated disc often shrinks over time or that symptoms ease. What matters is not just the size of the structural damage but the degree of nerve symptoms and function.
When surgery should be considered
- Bowel or bladder dysfunction (emergency)
- Weakness in the ankle/toes (paralysis)
- No improvement after 3+ months of conservative treatment
- Severe pain that makes daily life impossible
When it can be managed conservatively
- Pain is present but there is no paralysis
- Daily life is still possible
- Pain is gradually decreasing
- Improves with rest and posture correction
How we approach it at Yonsei SM
For a lumbar disc herniation, the key is not to “treat the disc alone” but to change its surrounding environment.
- Step 1: Calm (Circulation HD)
We settle the inflammation around the nerve and release nerves that have become stuck (adhesions). We approach this with injection procedures, without steroids. - Step 2: Activate (Circulation PT)
We wake up the weakened core (transverse abdominis, multifidus) and strengthen the gluteal muscles. We distribute the load that has been concentrated on the lower back. - Step 3: Integrate
You learn movements that protect the back, such as the hip hinge (bending from the hips) and deadlift patterns. We also correct how you sit and how you lift objects.
A lifestyle guide for disc patients
What to avoid
- Lifting objects by bending at the waist
- Sitting for long periods on a soft sofa
- Sitting with your legs crossed
- Sudden twisting motions
What’s recommended
- Lifting with bent knees (hip hinge)
- Using a chair with lumbar support
- Getting up to walk every 30 minutes
- Walking, swimming, and core exercises
Frequently Asked Questions
Are sciatica and a lumbar disc herniation the same thing?
Sciatica is a description of symptoms like “pain or numbness running down the leg,” and a disc can be one of its causes. We look at the distribution of symptoms together with the movements that trigger them. Sciatica Q&A →
If my leg is numb, does that always mean a disc?
Numbness can have many causes besides a disc, such as stenosis, fascial tension, or peripheral nerve problems. The location of the numbness and how it changes with movement are important clues. Leg Numbness Q&A →
Why does it hurt more when I sit?
Sitting for a long time increases pressure on the disc and can worsen the pain. We adjust your posture and rest patterns and, when needed, work on restoring function alongside this. Pain When Sitting Q&A →
When is back surgery necessary?
Surgery may be considered when there are emergency nerve symptoms (bowel/bladder dysfunction, progressive paralysis), or when there is no improvement despite adequate non-surgical treatment. We decide by looking at function and clinical course, not just imaging. Need for Back Surgery Q&A →
Does disc surgery completely resolve the problem?
Surgery is a way to address a specific structural problem, but if posture, strength, and movement patterns stay the same, pain can recur. Whether or not you have surgery, rehabilitation and correcting lifestyle patterns are important. Disc Surgery Q&A →
Can a disc show up on MRI but not hurt?
Imaging findings and symptoms don’t always match one-to-one. That’s why an assessment of your current symptoms and function is also needed. Pain With a Normal MRI Q&A →
Does walking help?
It depends on your condition, but walking short distances frequently often helps. If the pain worsens, the intensity and duration should be adjusted and an evaluation is needed. Pain With Walking Q&A →
How long does treatment take?
It varies depending on how long the pain has lasted and the degree of nerve symptoms. A stage to calm the pain and a stage to recover function may both be needed. Treatment Duration Q&A →
Related Articles
Wondering whether your disc herniation can be managed without surgery?
After an accurate evaluation, we’ll build a treatment plan tailored to you.
Book OnlineReferences
- Kreiner DS, et al. An evidence-based clinical guideline for the diagnosis and treatment of lumbar disc herniation with radiculopathy. Spine J. 2014;14(1):180–191. PMID 24239490
- Weinstein JN, et al. Surgical vs nonoperative treatment for lumbar disk herniation: the Spine Patient Outcomes Research Trial (SPORT). JAMA. 2006;296(20):2441–2450.
- Huang W, Sengupta DK. The influence of clinical symptoms on spontaneous resorption of herniated lumbar disc. Spine. 2014;39(14):1178–1183.
- Saal JA, Saal JS. Nonoperative treatment of herniated lumbar intervertebral disc with radiculopathy. Spine. 1989;14(4):431–437.